
Frank
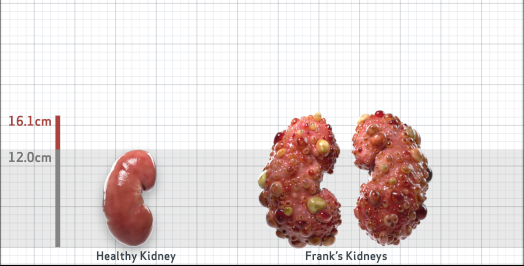
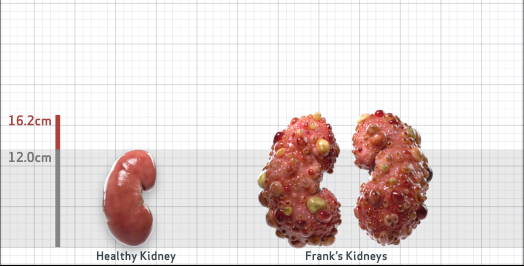
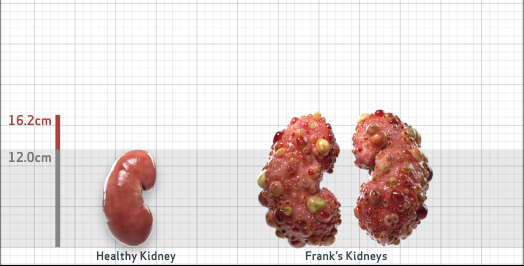
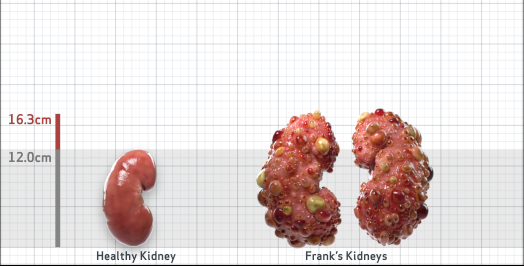
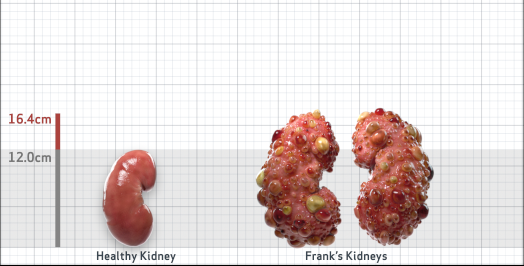
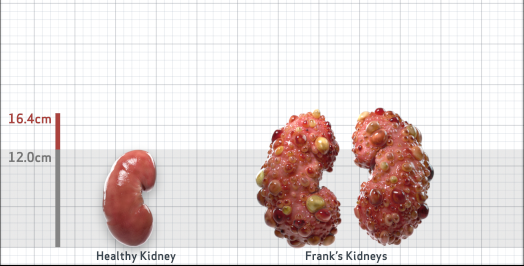
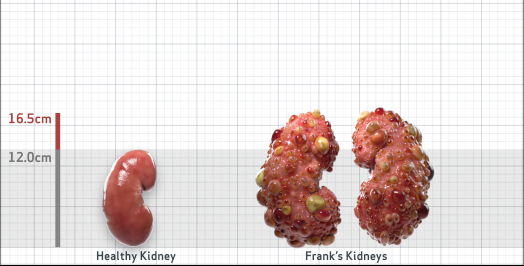
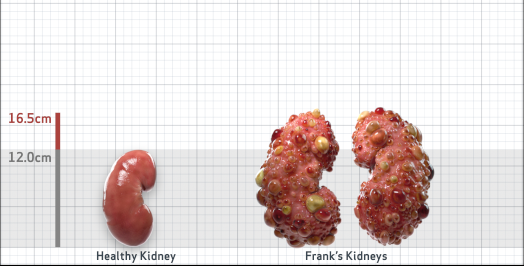
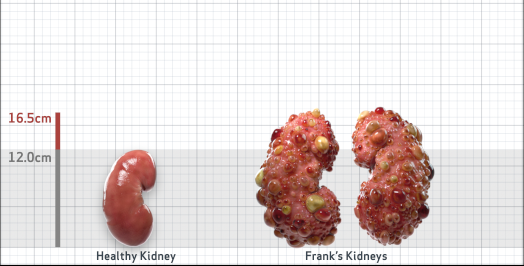
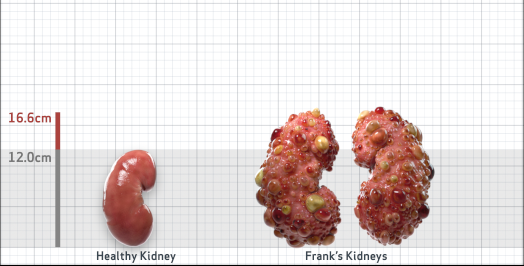
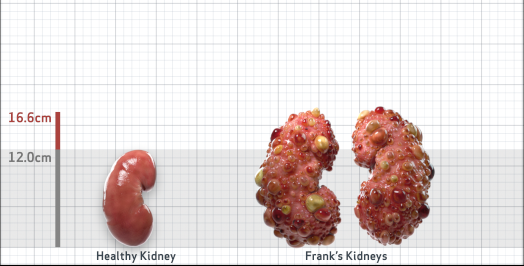
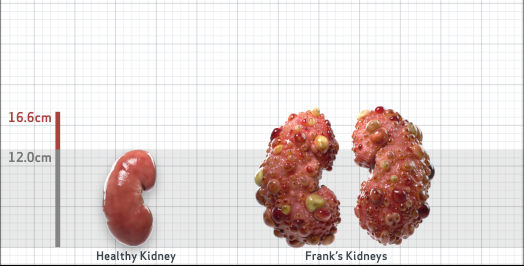
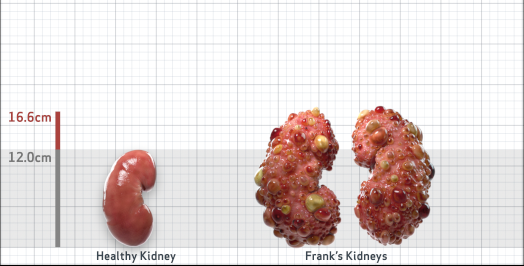
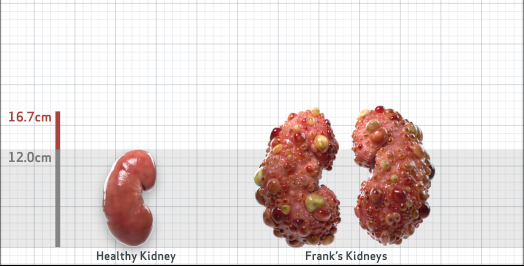
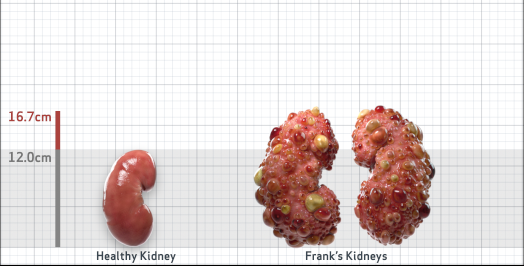
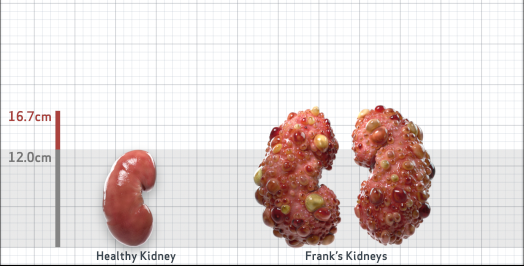
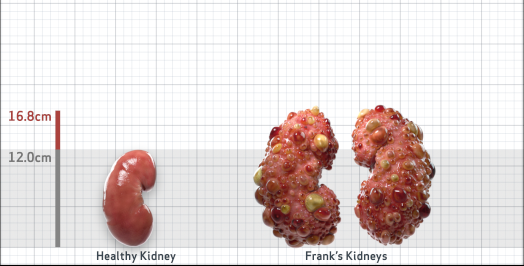
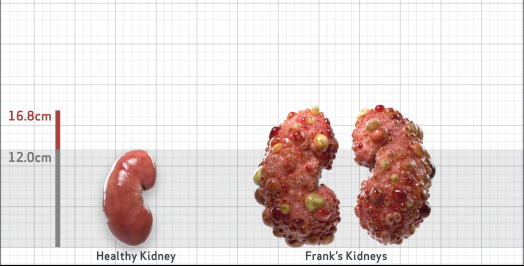
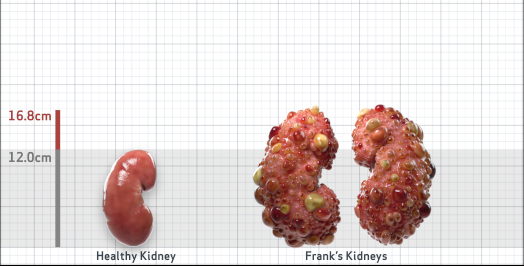
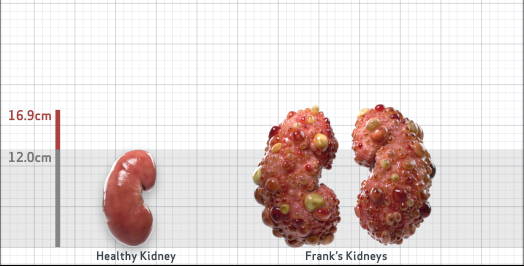
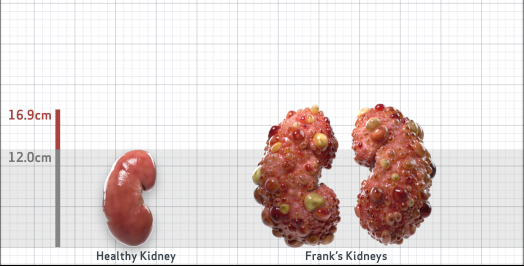
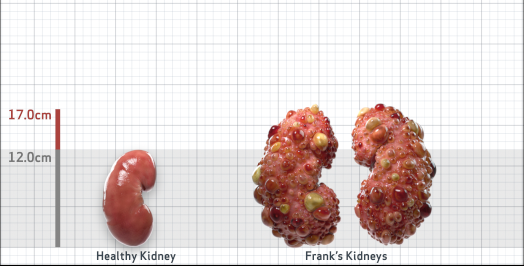
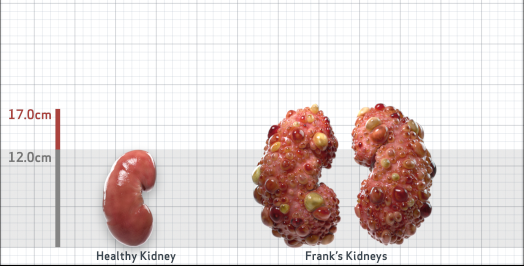
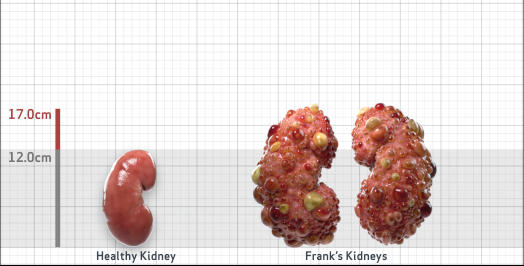
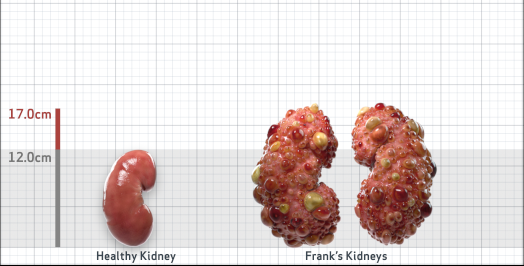
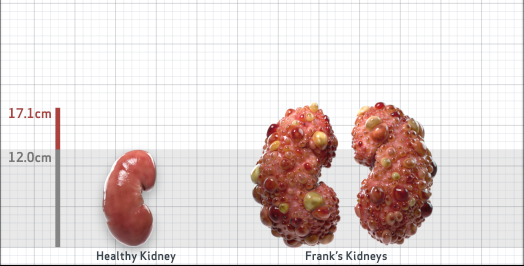
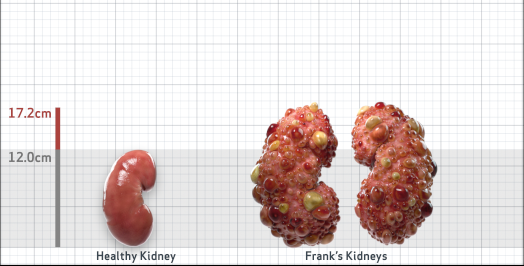
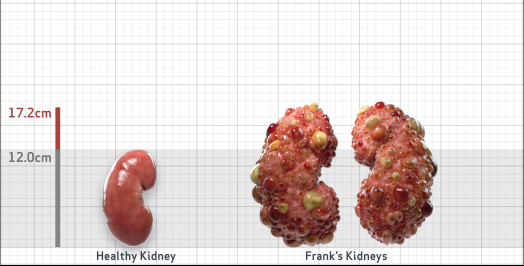
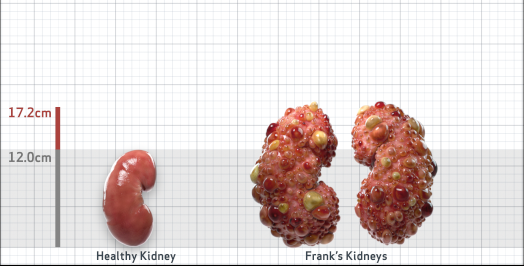
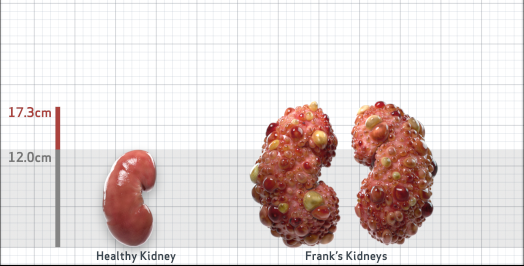
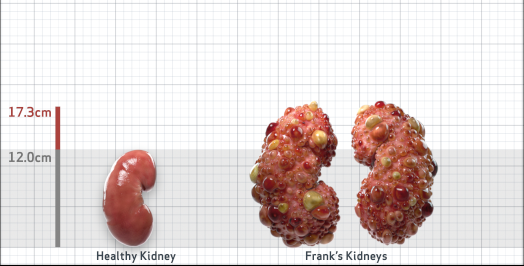
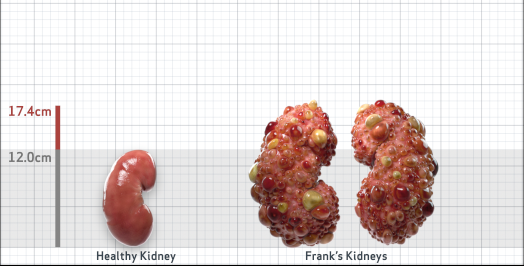
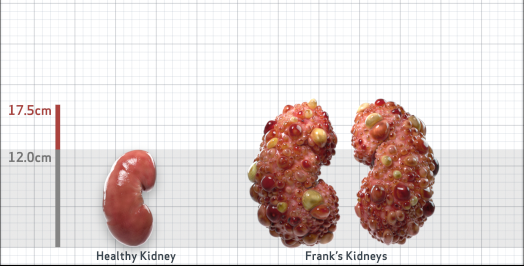
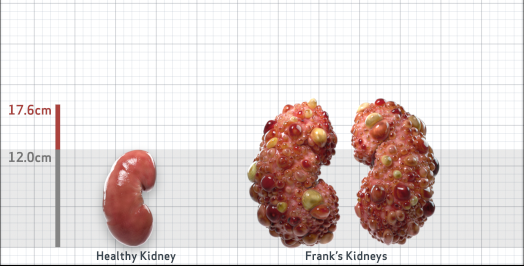
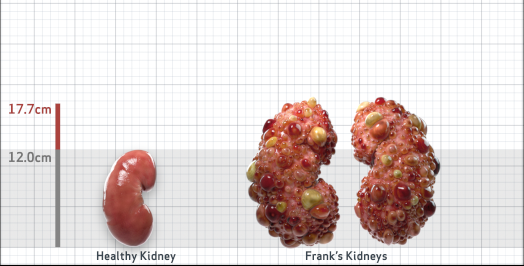
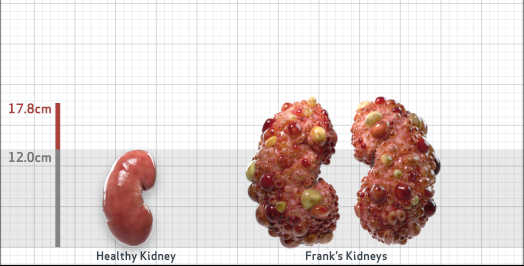
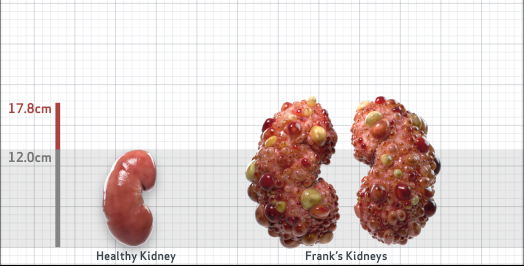
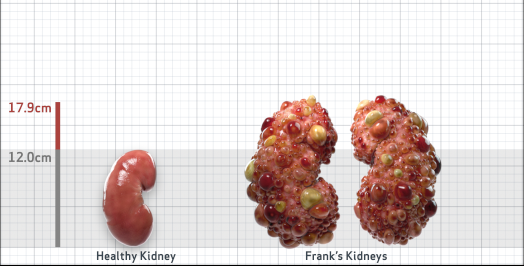
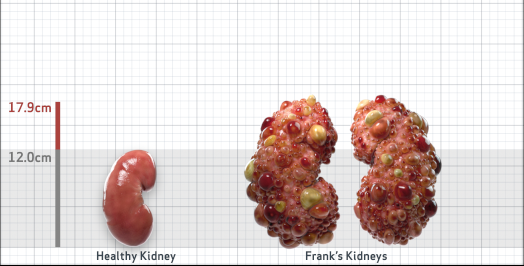
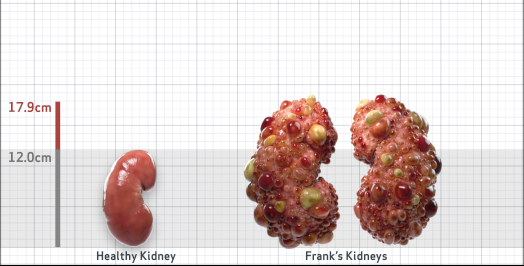
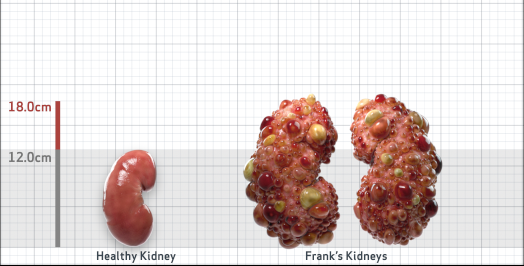
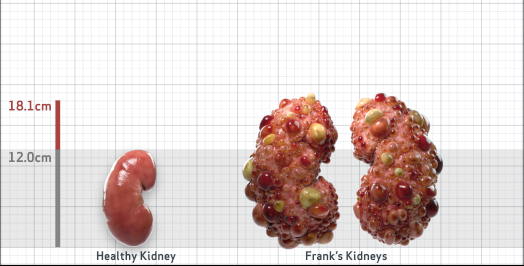
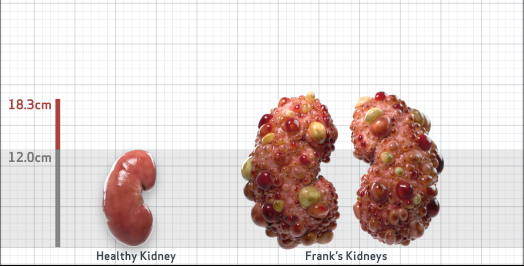
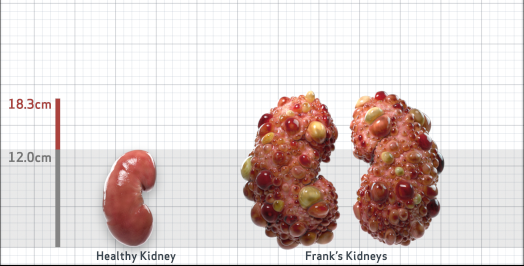
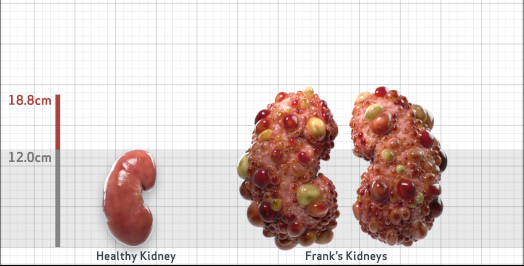
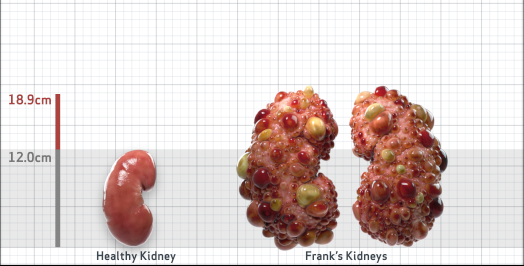
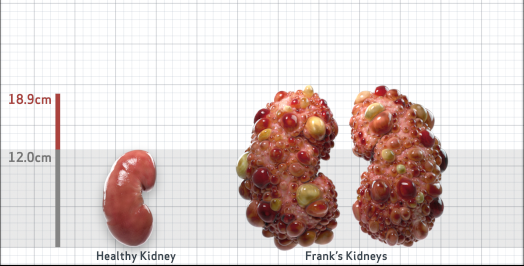
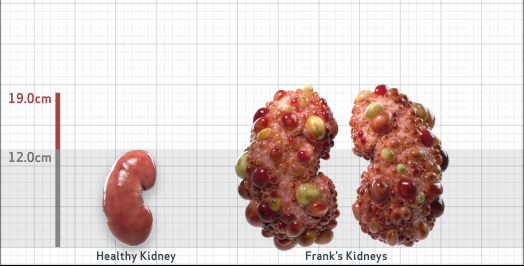
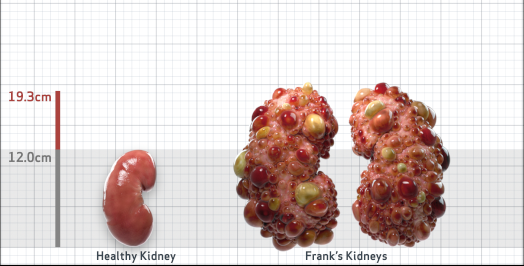
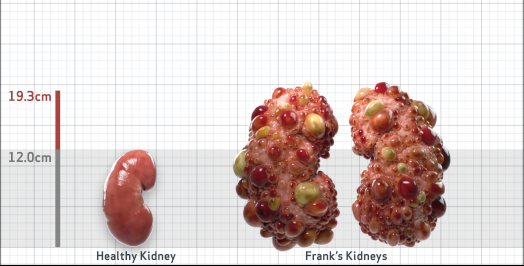
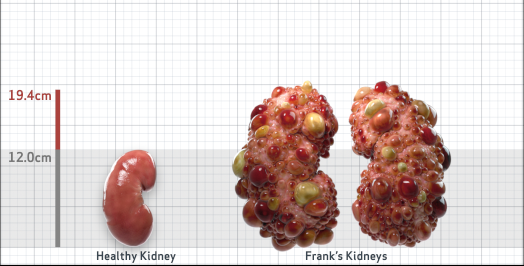
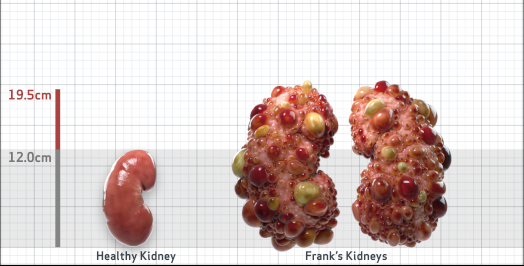
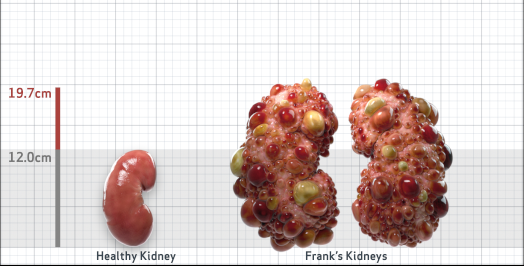
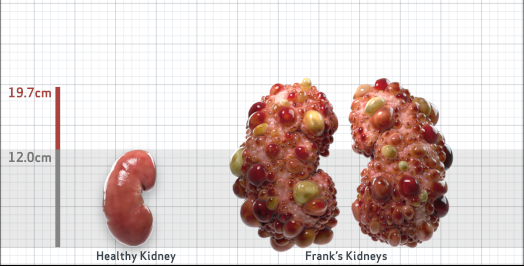
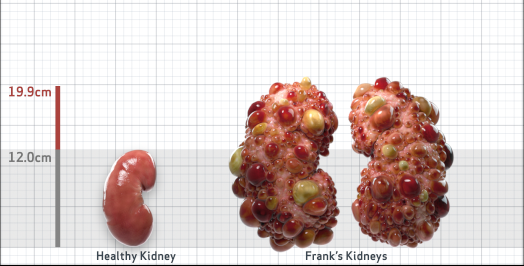
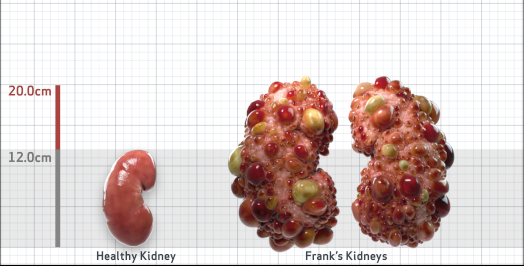
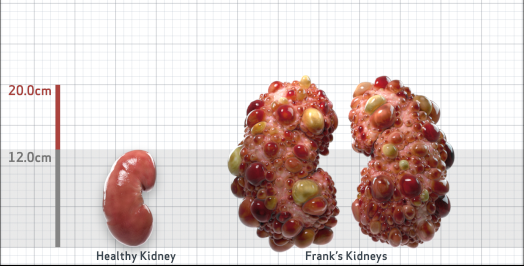
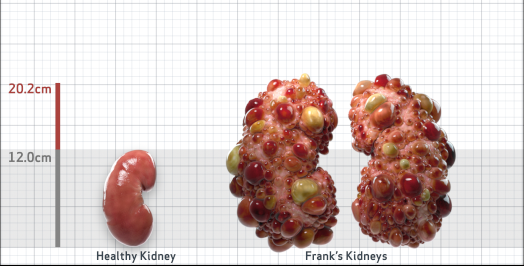
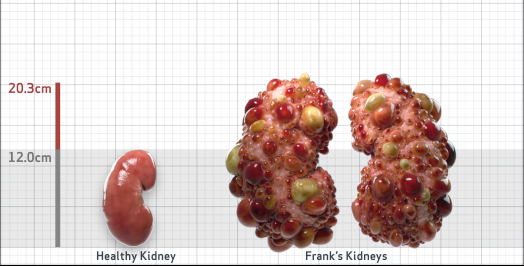
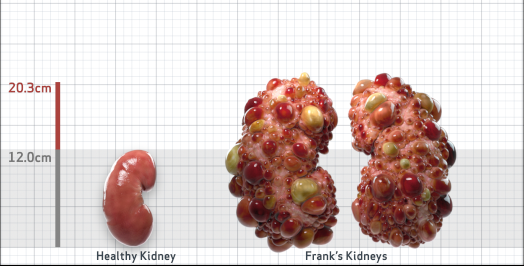
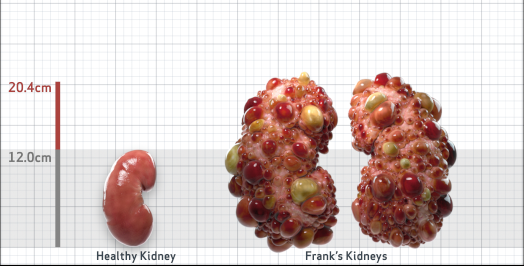
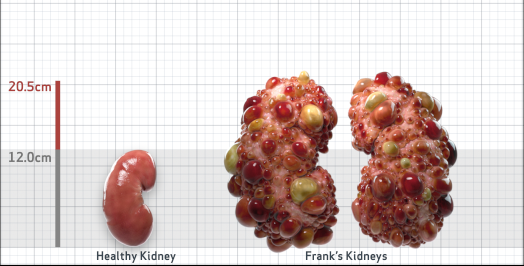
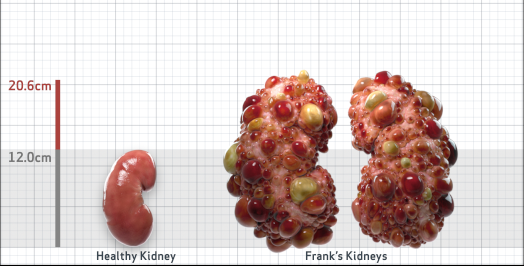
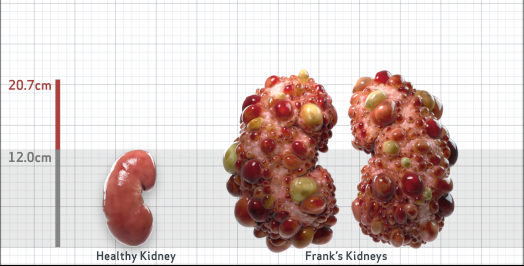
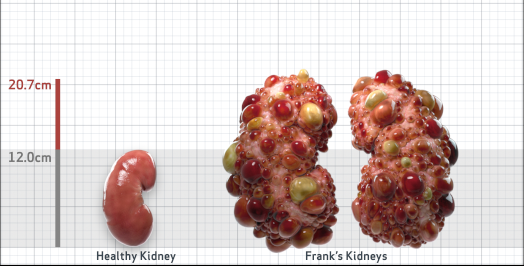
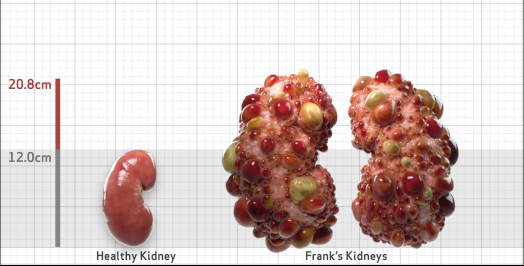
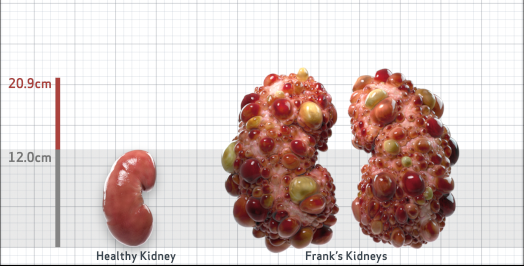
Frank is 52 years old and has been diagnosed with ADPKD by a kidney ultrasound. Frank is at risk for rapid disease progression, as indicated by the following risk factors: being male, rapid historical eGFR decline*, hypertension before age 35, urologic events before age 35, proteinuria/albuminuria, family history of ESKD by age 58, and TKV greater than expected for age. Let's take a closer look with some prognostic tools to confirm the risk of rapid disease progression and assess how rapidly his disease may progress.1,2
- Age52
- Height5'9"
- Weight181 lbs
- SexM
- Race (AA/O)O
Baseline Assessment2-7
- Serum creatinine (mg/dL)1.5
- eGFR (mL/min/1.73m2)52.8
- Ultrasound kidney length (cm)Not obtained
- Hypertension before 35?Yes
- Urological event before 35?Yes
- Family members with ESKD?Yes (58 yrs)
- MutationsNot available
- PROPKD ScoreNot available
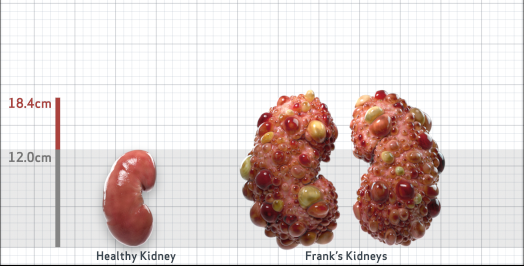
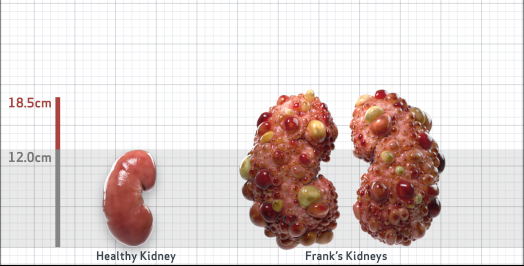
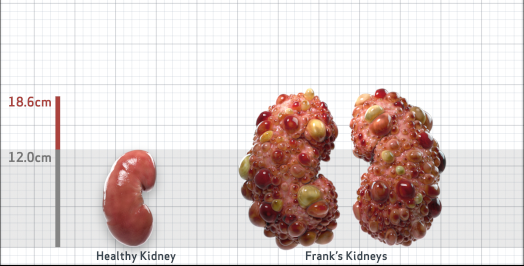
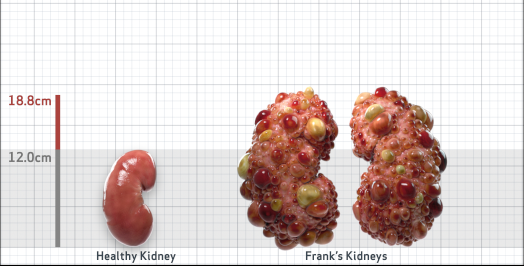
- htTKV (mL/m)1,669
- Other risk factorsProteinuria / albuminuria
- ADPKD Imaging Classification
Class 1D: High Risk for eGFR decline
4.5-6% estimated yearly percentage increase in kidney growth
ESTIMATED AGE AT ESKD61
MRI/CT SCANS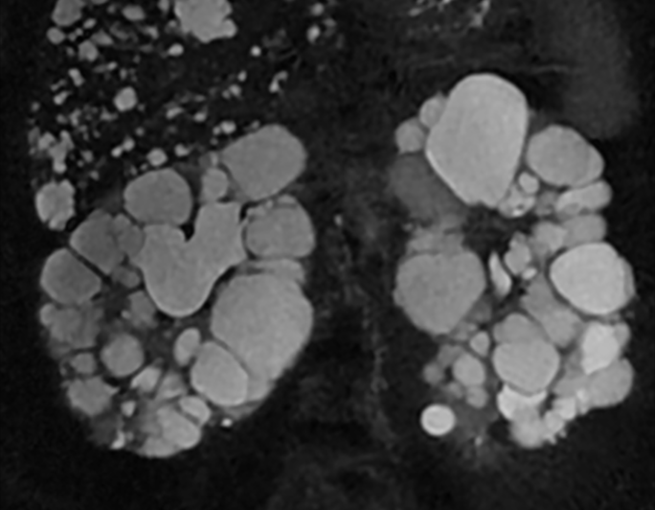

Disease Progression2-6,8-10















































Click on the flags below to walk through an assessment that confirms rapid disease progression risk and assesses how rapidly Frank’s disease may progress
*Confirmed eGFR decline ≥ 5 mL/min/1.73 m2 within a year and/or ≥ 2.5 mL/min/1.73 m2 per year over a period of five years.2
ADPKD=autosomal dominant polycystic kidney disease; eGFR=estimated glomerular filtration rate; ESKD=end stage kidney disease; TKV=total kidney volume; AA=African American; O=other; PKD=polycystic kidney disease; htTKV=height-adjusted total kidney volume; MRI=magnetic resonance imaging; CT=computed tomography; CKD=chronic kidney disease.Schrier RW, et al. Predictors of autosomal dominant polycystic kidney disease progression. J Am Soc Nephrol. 2014;25:2399-2418.
Gansevoort RT, et al. Recommendations for the use of tolvaptan in autosomal dominant polycystic kidney disease: a position statement on behalf of the ERA-EDTA Working Groups on Inherited Kidney Disorders and European Renal Best Practice. Nephrol Dial Transplant. 2016;31(3):337-48.
Wetzels JFM, et al. Age- and gender-specific reference values of estimated GFR in caucasians: the Nijmegen biomedical study. Kidney Int. 2007;72:632-637.
Irazabal MV, et al. Imaging classification of autosomal dominant polycystic kidney disease: a simple model for selecting patients for clinical trials. J Am Soc Nephrol. 2015;26:160-172.
Cheong B, et al. Normal values for renal length and volume as measured by magnetic resonance imaging. Clin J Am Soc Nephrol. 2007;2:38-45.
Imaging classification of ADPKD: a simple model for selecting patients for clinical trials. http://www.mayo.edu/research/documents/pkd-center-adpkd-classification/doc-20094754. Accessed January 09, 2019.
Cornec-Le Gall E, et al. The PROPKD score: a new algorithm to predict renal survival in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 2016;27(3):942-951.
Levey AS, et al. Definition and classification of chronic kidney disease: a position statement from kidney disease: improving global outcomes (KDIGO). Kidney Int. 2005;67:2089-2100.
PKD Charity. Fast Facts about ADPKD. The Polycystic Kidney Disease Charity. 2017. https://pkdcharity.org.uk/about-adpkd/just-diagnosed/fast-facts-about-adpkd Accessed January 09, 2019.
Rangan GK, et al. Autosomal dominant polycystic kidney disease: a path forward. Semin Nephrol. 2015;35(6):524-537.